MSK pain and burnout: two sides of the same workforce reality

Most organisations have made meaningful progress on burnout and mental wellbeing. Engagement surveys, resilience programmes, EAPs, manager training, and wellbeing initiatives are now standard for many employers.
Equally, many have invested in musculoskeletal (MSK) health - through ergonomics, health plans or PMI benefits. The issue is not lack of effort.
The issue is that these two areas are usually managed as separate problems, owned by different teams, measured in different ways - despite describing the same underlying strain on people at work.
Our data suggests that burnout and MSK pain are not parallel risks. They are two sides of the same workforce reality - connected signals of how sustainably work is functioning.
What the data is showing - and why it matters
Across large organisations, we see a consistent pattern: employees who report higher levels of musculoskeletal pain also report higher burnout scores.
What’s striking is not just that the relationship exists - it’s when it appears.
Burnout does not suddenly spike when pain becomes severe. It increases gradually as pain moves from mild to moderate to severe. Even low-level, everyday discomfort is associated with higher burnout scores.
In Vitrue Health’s dataset, this relationship is statistically significant (p<0.001), using the BAT (Burnout Assessment Tool), scored on a 0-5 scale.
This means that even low-level aches and discomfort are connected to psychological strain. By the time pain is labelled as “serious”, burnout is often already building in the background.
(It’s important to be clear: this is an association, not proof of direct causation. The relationship is likely bidirectional: pain influences stress, and stress influences pain.)
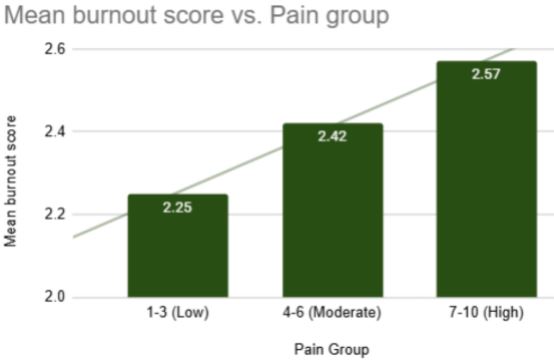
Burnout risk score (BAT, 0-5) vs. pain severity (Vitrue Health, 2025)
What this looks like in practice
Consider a typical employee experience:An employee starts the day with mild neck or shoulder discomfort. They feel slightly tense, take fewer breaks, and become more fatigued as the day progresses. Concentration drops. Meetings require more effort. Tasks that once felt manageable begin to feel draining.
From a benefits or people perspective, this may appear as stress, disengagement, or declining wellbeing. But physical discomfort is often a central part of the same story.
Now flip it around. A team is under pressure, deadlines are tight, and people are stressed. Shoulders creep up, posture worsens, muscles tighten, and pain sensitivity increases. Suddenly, what began as “work pressure” shows up in the body as pain.
In practice, you cannot neatly separate MSK from burnout. They feed into each other every day.
Why this changes how organisations should respond
If you only look at burnout data, you miss the physical side of the problem. If you only look at MSK risk, you miss the psychological side. Seeing both together changes what organisations can do.
With joined-up insight, organisations can:
- Spot early warning signs across both body and mind, before absence, claims or formal cases arise.
- Identify teams where pain-related strain is emerging, instead of assuming risk is evenly distributed.
- Understand how work patterns - such as back-to-back meetings, sustained screen time, limited recovery breaks, or prolonged laptop working - influence both burnout and MSK risk simultaneously
Crucially, this also changes outcomes.
Because pain and burnout reinforce each other, well-designed interventions can have compounding effects. Improvements in physical comfort, movement, and recovery can reduce burnout risk. Improvements in workload design, stress management, and recovery can reduce the escalation of pain.
Addressed together, organisations are more likely to see meaningful improvements across both domains.
From compliance to culture
Many organisations already invest significantly in employee wellbeing initiatives and benefits.
However, physical health and mental wellbeing are often managed through separate programmes, owned by different teams, measured against different outcomes. But this data suggests a more fundamental shift.
Supporting physical health and mental wellbeing should not be two separate programmes owned by different teams. It should be one joined-up culture of care.
That means thinking about how work is structured, how breaks are encouraged, how meetings are scheduled, and how movement is built into the day.
When organisations make this shift, they are not just preventing injuries or reducing burnout scores. They are designing work to be more sustainable - supporting performance, resilience, and health at the same time.
MSK pain and burnout are not competing priorities within a benefits strategy. They are connected signals showing how sustainably work is functioning for your people.
Supplied by REBA Associate Member, Vitrue Health
AI-powered MSK health - preventing pain before it hits claims and pathways