Why assumptions about MSK are costing employers

When we talk about ageing workforce strategy, musculoskeletal (MSK) health is rarely far from the conversation. The logic seems straightforward: older workers, more wear and tear, higher pain burden, greater cost. It's a narrative backed by intuition, grounded in general population health data, and embedded in how most organisations design and fund their wellbeing programmes.
But before we test that assumption against data, one caveat worth naming. The workers most affected by MSK pain may not be in any working population dataset at all. Employees with severe, chronic conditions are disproportionately likely to leave the workforce early - through ill-health retirement, long-term absence, or finding desk-based work unsustainable.
The older workers in Vitrue Health’s platform data sample are, by definition, those well enough to still be working. Every difference we observe between age groups is almost certainly an underestimate of what's actually happening.
With that in mind, here is what a sample of more than 20,000 desk-based workers from Vitrue Health’s platform data actually shows.
Older workers do not report significantly higher pain
The pain scores are almost identical.
Here's the finding that surprises people most: older and younger workers report nearly the same average pain scores (4.57 vs 4.41 out of 10). The proportion experiencing high pain is similarly close - 19.9% in the 50+ group versus 18.4% in those under 50. Neither difference is statistically significant.
In other words, the data does not support the idea that older workers simply have a higher raw pain burden. The raw pain burden is broadly comparable across age groups.
The same pain creates different cost profiles
The more important difference is not how much pain people report, but how that pain shows up.
In workers aged 50 and over, pain is significantly more likely to disrupt sleep (43.1% vs 36.1%) and drive healthcare use. Over half - 56.9% - had consulted a healthcare professional about their pain, compared to 44.1% of younger workers. They were also significantly more likely to take time off: 24.0% versus 18.3%.
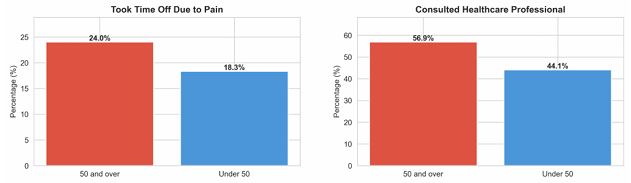
Figure 1: Pain-related absence and healthcare use by age group
In workers under 50, pain is significantly more likely to hit productivity (23.1% vs 15.9%) and concentration (28.8% vs 17.8%).
The same pain intensity is creating two distinct cost profiles.
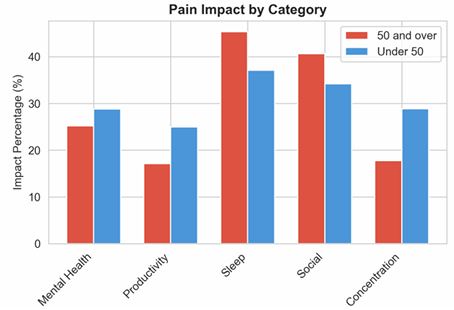
Figure 2: Reported impact of pain on work and wellbeing by age group
For older workers, the cost shows up in healthcare spend and absence - visible, measurable, and relatively easy to act on.
For younger workers, the cost is more likely to show up as presenteeism: employees are still at their desks, but pain is affecting their ability to concentrate and perform. This rarely appears in absence reports, may not trigger clinical support, and can accumulate quietly across a workforce.
What this means for benefits design
The implication for benefits leaders is clear: ageing workforce strategy should not be built around the assumption that older employees simply hurt more. The more useful question is how pain affects different groups, and what kind of support each group is most likely to need.
Invest in younger workers earlier: Pain in under-50s is less likely to show up through healthcare use or time off, but more likely to affect productivity and concentration. That makes early intervention especially important, because the cost may be building long before it becomes visible in absence data.
Support what older workers are already doing: They are engaging with healthcare, adjusting their behaviour, and taking action. Benefits that meet them where they are - accessible physiotherapy, sleep support, return-to-work programmes - will have higher uptake and better ROI.
Don't ignore the pain-productivity intersection.
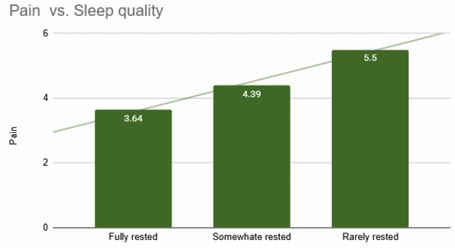
Figure 3: Pain-related sleep disruption by age group
Over 43% of older workers report sleep disruption from pain. Sleep remains consistently under-addressed in workplace wellbeing benefits stacks, yet it sits at the centre of recovery, cognitive performance, and long-term absence risk.
Use data to segment, not to stereotype: Age alone is a blunt instrument. Organisations with access to workforce-level MSK data can identify where the real burden sits - by age, role, location, or department - and invest accordingly.
The opportunity
The ageing workforce conversation in the UK is only going to intensify. With the state pension age rising and more employees working into their 60s, the pressure on benefits professionals to make better, more targeted decisions about MSK support will only grow.
The organisations that manage this well will be those that understand the actual shape of risk in their workforce - not the assumed shape, and not just the visible portion of it. That starts with asking better questions of the data, and being honest about what the data cannot yet see.
Analysis based on a sample of 20,000 desk-based workers from VIDA - Vitrue Health’s platform data. Statistical significance assessed at p < 0.05.
Supplied by REBA Associate Member, Vitrue Health
AI-powered MSK health - preventing pain before it hits claims and pathways





