Equal by design, unequal in practice: the gender gap hiding in workplace MSK support

Most workplace musculoskeletal (MSK) and wellbeing strategies are built around a simple and well-intentioned principle: offer the same benefits, guidance and access to support to everyone.
This approach aligns with how equality in benefits has traditionally been interpreted, and with the direction of European pay transparency legislation, which emphasises equal access to workplace benefits. In practice, however, equal access does not always translate into equal outcomes.
For benefits and wellbeing leaders, this raises a practical question: how do you demonstrate fairness and effectiveness when outcomes diverge, even where access is equal?
Across thousands of desk-based MSK assessments conducted in 2025 (Vitrue Health, 2025), one pattern stands out clearly. Women are more likely than men to report MSK pain related to their working day, and when they are in pain, they consistently rate that pain as more severe.
This isn’t a marginal effect that disappears with larger datasets. It’s a stable, replicable disparity observed across thousands of assessments, industries, geographies, ages and seniorities. That matters because MSK pain remains one of the most common drivers of absence, productivity loss and healthcare spend in desk-based organisations - and is an area where employers already invest heavily through wellbeing and benefits programmes.
If a “same-for-everyone” approach to MSK support consistently delivers different outcomes for different groups, then a strategy designed to be neutral can, unintentionally, reinforce inequality of impact.
What the data reveals about MSK outcomes
The data below examines whether this assumption holds in practice for one of the most common areas of benefits investment: workplace MSK wellbeing.
In 2025, women reported:
Higher average pain severity than men (around 35-40% higher on a 0–10 scale)
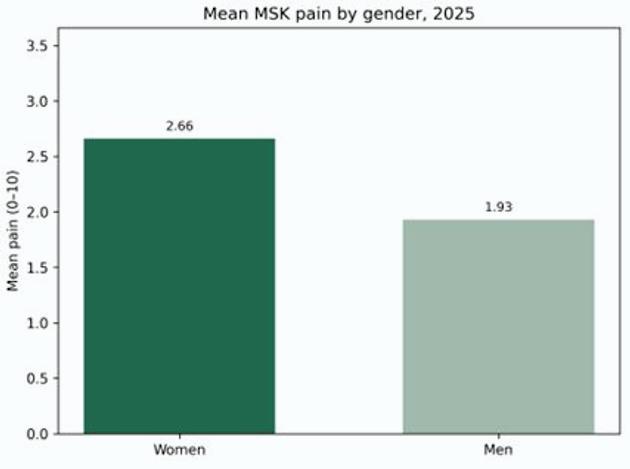
Fig 1. MSK pain by gender (Vitrue Health 2025)
Higher pain prevalence (a greater proportion of women were in pain at the time of assessment)
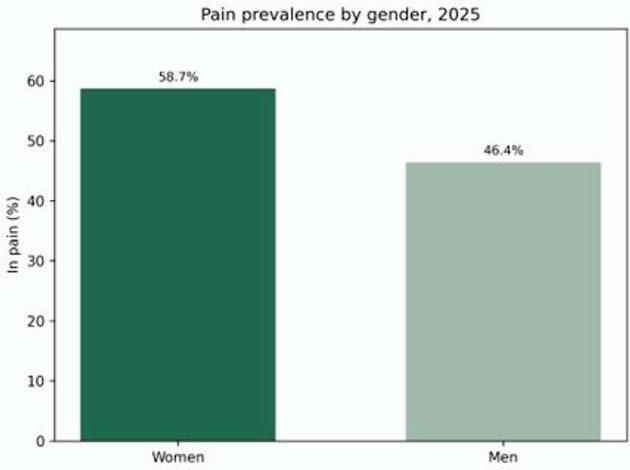
Fig 2. Pain prevalence by gender (Vitrue Health 2025)
In practical terms, women are both more likely to experience MSK pain at work and, when in pain, to experience it more intensely. This directly tests the assumption underpinning many health and wellbeing strategies: that equality of access is sufficient to achieve equality of impact.
Importantly, these differences were observed within organisations where men and women had access to the same MSK wellbeing benefits and assessment pathways, removing unequal provision as a primary explanation.
Where the disparity concentrates
The gender pain gap is not evenly distributed across the body. It concentrates most strongly in the neck, shoulders and mid-back.
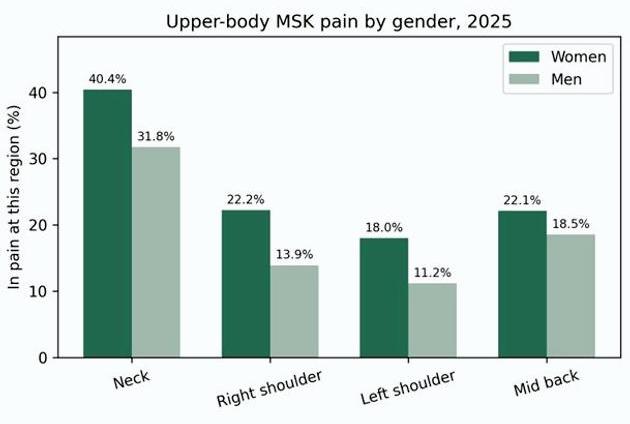
Fig 3. Upper-body MSK pain by gender. (Vitrue Health 2025)
The concentration of the gap in the upper body is not incidental. These are regions where desk-based work exposure and the effectiveness of MSK support make the greatest difference.
When a single, standardised approach is applied to varied working patterns and physical needs, differences in outcome become most visible here.
What this means for organisations
Vitrue’s 2025 dataset points to a clear conclusion: workplace MSK outcomes are not experienced evenly across genders. A purely gender-neutral approach - providing the same support, in the same way, with the same escalation thresholds - can systematically underperform for the group experiencing higher levels of pain, particularly in desk-based roles.
For benefits and wellbeing leaders, the implication is not that strategies need to become gender-specific by default, but that they need to become more responsive to where risk and impact are actually concentrated.
In practice, this often means looking again at how existing MSK pathways perform across the workforce. Many organisations already invest in a broad mix of support - such as gym memberships, yoga or movement classes, onsite or virtual physiotherapy, private medical insurance, and health or cash plans. The data here suggests that availability alone is not the issue. The question is whether these pathways are being accessed early enough, targeted appropriately, and delivering comparable outcomes across different groups.
For most organisations, addressing this gap does not require new benefits, but clearer prioritisation of how existing MSK support is designed, targeted and governed.
- Design MSK support for variation, not averages: Rather than assuming standard provision works equally well for everyone, review whether your MSK support - across equipment, guidance and access pathways - genuinely accommodates variation in body size, working patterns and day-to-day demands. Where support relies on optional adjustments, ensure these are normalised and easy to access, rather than treated as exceptions.
- Target early intervention where outcomes diverge most: The data shows that outcome gaps are largest in upper-body pain linked to desk-based work. This makes it a logical focus area for targeted early intervention - whether through brief movement support, behaviour change prompts, or faster access to clinical guidance - rather than relying solely on generic wellbeing content or late-stage escalation.
- Govern MSK strategy based on outcomes, not just uptake: To understand whether an MSK strategy is working as intended, benefits leaders need visibility beyond overall engagement metrics. Tracking outcomes by gender and by pain region helps reveal who is benefiting in reality. Where disparities persist, this provides a clear signal to revisit both how support is delivered and how effectively employees are enabled to tailor it to their needs.
Key takeaways
- Vitrue’s 2025 desk-based assessments show a consistent and systematic gender gap in workplace MSK outcomes: women report both higher prevalence of pain and higher pain severity than men (around 35–40% higher on a 0–10 scale), with disparities concentrating in upper-body pain linked to desk-based work.
- As scrutiny around gender pay equity and equal access to benefits increases - including through European pay transparency legislation - employers may need to demonstrate not just consistent provision, but consistent impact from MSK and wellbeing strategies.
- Addressing this does not require gender-specific benefits by default. It requires MSK strategies that are more responsive to where risk and impact are actually concentrated, with earlier and more targeted support where outcome gaps are largest.
- Governing MSK and wellbeing strategies based on outcomes - including tracking impact by gender and by pain region - provides a more robust foundation for demonstrating fairness, effectiveness and value under increasing regulatory and stakeholder scrutiny.
- Digital MSK assessment approaches can support this shift by linking pain severity, location and work-related risk signals, enabling targeted intervention without relying on assumptions based on gender alone.
As organisations prepare for increased transparency and scrutiny in 2026 and beyond, understanding where benefits deliver equal access but unequal outcomes will become an increasingly important part of MSK and wellbeing strategy.
Supplied by REBA Associate Member, Vitrue Health
AI-powered MSK health - preventing pain before it hits claims and pathways